Hospitals Can Be Like Any Other Office
Same institution but made up of different sections seeing the less of the bigger picture and functioning interdependently. Sounds like most organizations to me as each department has it’s own business to do to keep the institution running. I think most people outside the health care industry forget this tiny detail whenever they ask for their medical records post discharge. A single medical record is the sum of the different departments that labored through making those pieces of paper. I work in one department, the pathology section where all the background work gets done while the ones at the front lines get most of the spotlight.
Note: I like to do a show and tell portions of the post just so anyone that comes by may get a trivia for their time reading.
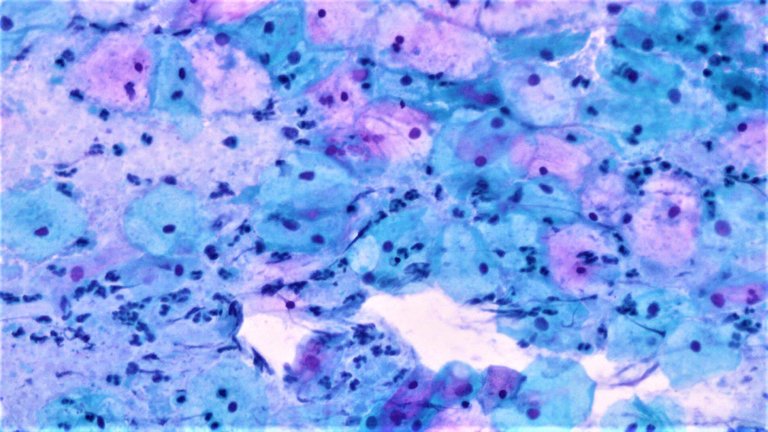
Unrelated to the content but I just wanted to flex the image I took from my first batch of pap smears examined. Taken from the cervix, those tad pole like structures are sperm. Those tiny dotted parts are neutrophils reacting to an infection possibly reacting also to sperm as a foreign body.
My co-residents and medical laboratory staff often get misunderstood as we have the most specialized and least observable work environment. Staff from different departments would just look at the small window where results are released not minding the background labor that’s been going on inside the walls. They’d think the machine just prints the results as soon as one plugs in a test tube to analyze the sample. They also think that after submitting some tissue specimens, the results would just get conveniently published with a clear cut diagnosis.
A lot of the minor details that happen in the lab to keep thing running aren’t on the minds of the people that make up other departments. It’s all alien to them how machine X used for this test is better than machine Y for the same test, how quality assurance checks need to be made, and doubting the specimen submitted. After all, each department is like it’s own cubicle minding it’s own business and only complains when some other department’s responsibility lags.
Ok, so why all the build up on those paragraphs, what’s the point? It’s just what I think after the recent changes in policy our department had to go through from weeks of freedom from the other mundane labors that be.
We recently had to allocate some man power on the triage to help with the lack of personnel to do it. The bulk of the triage work is classifying whether a patient should be sent to the clean ER or covid ER using a mechanical checklist. It’s a no brainer job for any health care worker but stressful as you also have to coordinate with multiple departments to get some of it done. A nurse can do it but it seems our admin insists on having doctors doing the task for reasons unknown.
To put it in another perspective, any health care personnel can do it with some training and all it takes is some time getting used to. You just ask the patient what’s on the checklist and classify if they qualify for the clean ER or covid ER. Then contact the department that’s going to handle their case to see if there are any available rooms to accommodate them (Surgery for trauma/burn patients, Internal Med for Kidney problems and etc). The stress comes from people that don’t pick up the phone and irate folks/patient.
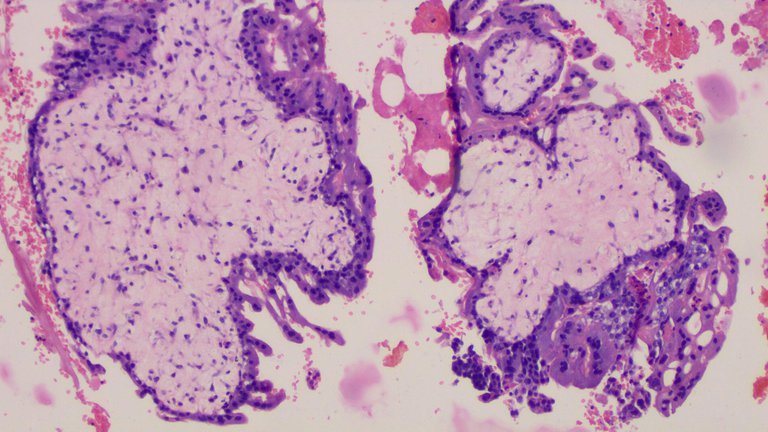
This is a placental tissue showing avascular villi. We often receive cases of products of conception (from miscarriages and diagnostic curettage) to confirm and document that pregnancy took place and correlate it with age. We look at the villi to see how mature the placenta may have been. Judging from how large, avascular, and how these have trophoblastic proliferations on the sides indicates this was probably a placenta on it's first trimester (assuming I haven't looked at the clinical diagnosis).
For reasons unknown, the admin just can’t hire another triage officer to do this task so the burden is placed on the existing departments to provide one resident for each shift as a sacrificial lamb in the guise of learning. Note, residency training did not include us signing up for this task, we don’t learn a lot from our time on the shift and we are more deprived from what we should be learning like actually doing our actual specialized work.
So Pathology department has been exempted from the work since January and only until recently did they start eyeing our department to comeback into the fold after another department got pulled out from duty due to allocating more manpower to the covid ward and some departments be on quarantine. See this is where the fun part about residents meeting trying to negotiate why we don’t want to do the triage, it’s not part of our training and we have the few people on our roster to do it. We already do two to three tasks meant for one person each task to compensate before this happened.
Because we are the background workers that magically pop some results from the lab or histopath, most of our work goes underappreciated. Another perspective is, we got basic training as a doctor so we can do the stuff other departments do with some minor reorientation to their specialties but the same can’t be said for any department willing to take on our tasks. That’s just how specialized the pathology department. I shed a lot of what I learned from medschool and internship to suit pathology, the only thing left for me is doing the bare minimum of what is expected of a doctor when manning a ward, the rest have gone into the abyss. It’s easy to relearn those stuff again but if other residents tried to learn our stuff they would need some months before getting the hang of the work especially if they aren’t a medical technologist for their premed degree.

Right colon mass, it's the mass at the 20cm mark on the right side of the image. Looks intimidating to dissect but just needs some getting used to. One just needs to take the edges of the specimen as margins and sample the mass. If one can find some lymph nodes, we take at least 12 of them to make an adequate staging of the cancer.

This is the bottle that came with the above specimen. As you can see the levels of formalin placed on the bottle triggered my pet peeve. Naturally the red part you saw on the specimen is unpreserved portion of the tissue due to inadequate formalin used on the bottle. We have been telling the surgical residents time and time again to drown their specimens instead of dipping them to make it look full.
Pathology has it easy. That’s what the other departments think as we don’t look like our work is difficult. Seems reasonable to some degree, most of my work ends up looking at a microscope in a comfy air conditioned room or laboring at the histopath section smelling formalin soaked specimens and making friends with corpses prior to doing autopsies. The thing is, once a case gets assigned to us we will be assigned to it from start to finish and even years after the result is published. Once a resident goes off from duty, it’s out of sight out of mind.
I get called in the middle of the night on cases that need urgent follow ups. Some cases are just that difficult to diagnose even with adequate immunohistochemical stains (which may not happen as the patient can’t afford them, third world issues). Whenever I’m talking to a resident from a different department and some silly thing as why are the results too slow to be signed out, I just have it in my head that these people don’t know jack shit on most of the work being done to make those results happen.
Anyway, the triage sucks, we got to man it for 8 hours and those 8 hours are lost doing mundane tasks which could’ve been allocated for training. Each department has their own thing to worry that it makes every department lose track of the bigger picture but at least we can still function interdependently to keep things running. The change in schedule caused some friction with other departments and even in ours internally. Senior politics has it’s own drama where some people just don’t want to take on the work expected of their pay grade because they are way above the task.
If it were just me not in specialized training, triage work is just a walk in the park, easy money and out of sight out of mind once the shift ends. But then I’m in a specialized training program where after triage I have other responsibilities to the department and this isn’t covered in my salary. It’s almost August and I still have 0 salary since I started working for this institution, not really a problem as I have managed to live off with a frugal lifestyle, I think I could still keep surviving for an entire year provided I do some commissions for art on the sidelines (my digital art ain’t that great but traditional portrait sketches and small design works can generate me some income if I squeeze that in my sched.) I have always thought what I’m doing is consenting to modern slavery but I get a nice certificate to put on my credentials in the end. I still love my work and see value in it, for the greater good type of value.
Posted with STEMGeeks
People don't know the value of a thing until it isn't available. Lab work is a pillar of research. It's undervalued and most of the time thankless. However, you have to have surgeons like you need to have technicians and analysts.
I have to write that maybe I'm naïve about testing, but I would have figured that testing was outside of patient costs. I mean, if a doctor needs the analyses can't it just be done? I never worked in hospitals or in pathology but I have worked in research and production water chemistry labs. We never broke down costs to that degree.
We did, though, have to present project experiments. Maybe that's similar in a way. The huge difference, of course, being that it's water and not people.
Regarding patient's costs, it will depend on the institution's policy on how they handle who pays the costs, sometimes private insurance or public health insurance covers it but I think of the process as patient still pays for it under a different method I mean, their taxes go to the public health insurance and their money is still used to pay for private insurance policies.
From experience, lab costs take up the top 2 or 3 spot for hospital bill expenses for long staying folks. 3rd world countries have different approaches to health care, we don't have that luxury of insurance companies backing our health care needs, most people anyway, so a lot are out of pocket expenses.
We need each department to run as a whole and that's a fact. Just that each section has their own world to mind that they don't really get what other sections are doing at the same time.
If the patient can't afford it, it can't be done because the costs just goes back to the hospital and its a business institution still. This is a reality that some cases just go untreated or under diagnosed just cause the patient can't afford it.
Ok. It makes sense. I worked in a steel mill where I helped to set up their water treatment systems. I lumped all the costs of lab equipment, repairs, materials, reagents, and bulk treatment chemicals into that system's overall operating costs.
Sampling and testing occurred at the frequency required by regulation and vendor recommendations. So, if extra testing was required who would pay for it? The steel mill would.
Thanks for the conversation. It looks like costs aren't too different after all between our work.
Your welcome and thank you for the input.
I pay little attention to costs after being desensitized with how limited resources is a common occurrence. Some things you just have to let it go and let it be someone else's problem given the limited resources you already have.
Congratulations @adamada.stem! You have completed the following achievement on the Hive blockchain and have been rewarded with new badge(s) :
Your next target is to reach 20 posts.
You can view your badges on your board and compare yourself to others in the Ranking
If you no longer want to receive notifications, reply to this comment with the word
STOPYour pictures remind me of my childhood: my father was a pathologist. Sometimes after school, I'd wait at the lab to go home with him later. I remember the specimens and slides well
I've would've probably set out my life path to be a pathologist early on if I had been exposed to the wonders of the microscope like that. Though I doubt that the smell of formalin was pleasant if you also had a lot of lab exposure.
The place did smell rather foul. I did want to do something scientific as a child but sadly, life got in the way
Ah, the glorious days of unpaid internships and perpetual terrible personnel management.